Archive for May 2024
Access Closure: Case #1
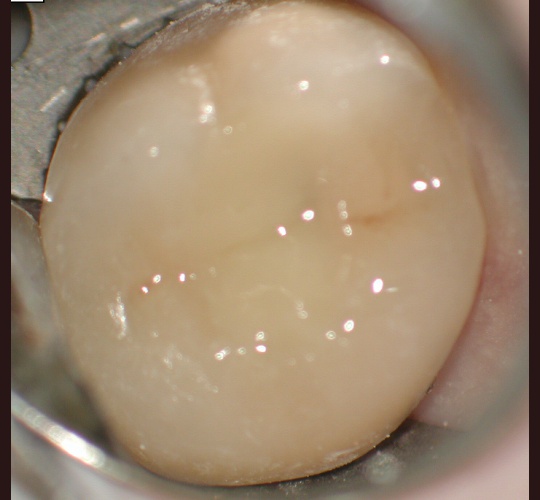
When the crown is still intact and in good shape the root canal access opening can be sealed and the crown can be reused. Modern access shape outlines should not overextend and weaken the peri-cervical area. These shapes do not conform to endodontic textbook teachings. These shapes are to be done by qualified microscope using…
Read MoreEndodontic Microsurgery: Case #5 – Intentional replantation (not so common procedure)

In area where endodontic microsurgery is not possible due to various reasons the tooth can be extracted, treated and replaced back into the mouth. This tooth was treated and did not respond well to treatment was to be extracted but we were able to remove the tooth and seal the untreated anatomy with our MTA…
Read MoreEndodontic Microsurgery: Case #4

This patient has persistent pain after root canal therapy performed 2 years earlier. Due to her new bridge she did not want a retreatment. It was a reasonable choice for microsurgery to be performed. A scalloped incision was made to prevent gum recession and to hide the scar due to her high lip line. Pain…
Read MoreEndodontic Microsurgery: Case #3

Patient referred for a consultation and treatment of a radiolucent (dark area) at the end of the root with pain and swelling. A 3-dimentional image (CBCT) was taken during his consultation appointment. Reviewing the images showed two roots in a lower first. The CBCT was an invaluable tool is aiding our diagnosis and treatment. A…
Read MoreEndodontic Microsurgery: Case #2

The root canal was performed 6 months prior by an excellent endodontist a notation that there was a possible third canal present during the initial root canal but they were unable to negotiate it. Slight pain persisted and an apicoectomy (root canal microsurgery) was decided upon due to its complex root anatomy. As expected 3…
Read MoreEndodontic Microsurgery: Case #1

Very rare and unique. Patient referred for a consultation and treatment of a radiolucent (dark area) at the end of the root. A 3-dimentional image (CBCT) was taken during her consultation appointment. Reviewing the images showed two roots in a Maxillary central incisor (upper front tooth) which is a rare occurrence. The CBCT was an…
Read MoreEndodontic Retreatment: Case #5 – Retreatment of initial root canal done 30 years earlier.

Problem 7 mm periodontal pocket on the buccal side with slight pain to biting. His general dentist felt that the tooth may be fractured and referred the patient to determine if an extraction is necessary. During examination we determined that there was a missed DL canal that is challenging to locate. This type of tooth…
Read MoreEndodontic Retreatment: Case #4 – Retreatment of initial root canal done 12 years earlier

Problem recurrent infection with swelling due to the original root morphology was a “c-shape canal did” with lots of untreated canal space and not treated to the bottom of the canals. The root canal was retreated and all canals were located, cleaned and medicated with CaOH. The root canal was sealed with gutta percha and…
Read MoreEndodontic Retreatment: Case #3- Retreatment of a recent root canal performed 2 weeks earlier.

During his consultation It was determined that there is untreated canals present and initiated retreatment. With the aid of the microscope 5 canals were present, treated and sealed. Both the patient and his general dentist were extremely pleased with the outcome.
Read MoreEndodontic Retreatment: Case #2- Retreatment of initial root canal done 15 years earlier.
Problem recurrent infection with swelling due to the original root canal 15 years earlier has an untreated MB2 canal. The root canal retreatment was initiated and an MB2 canal was found, cleaned and medicated with CaOH. Her symptoms immediately resolved and the tooth was complete by sealed with gutta percha, AH+ sealer and the crown…
Read More